
#What is Wellens syndrome?
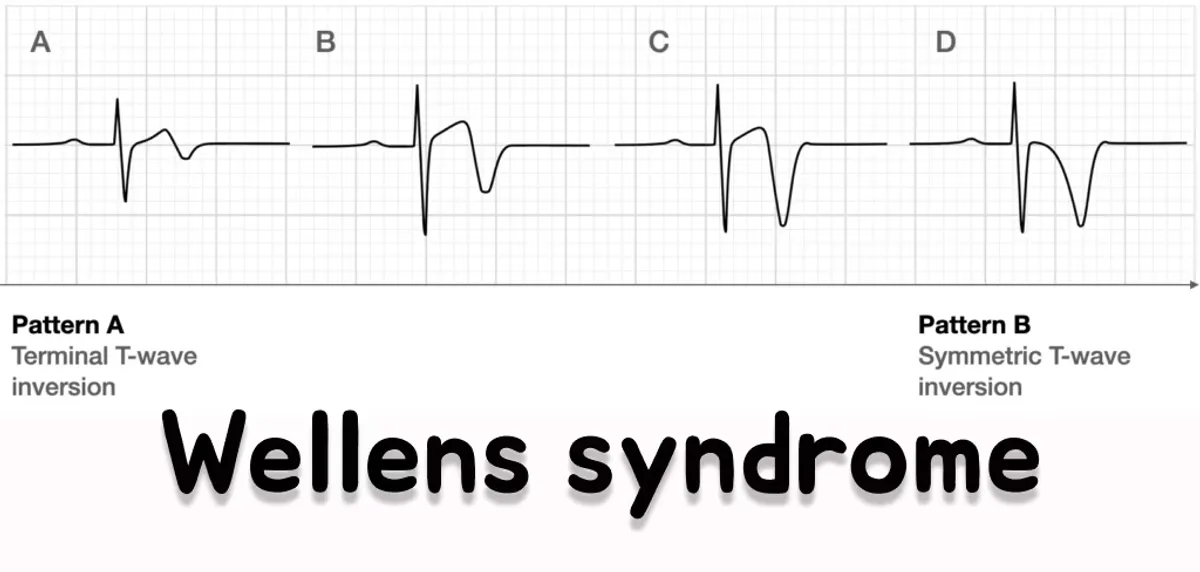
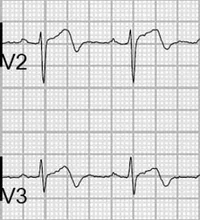
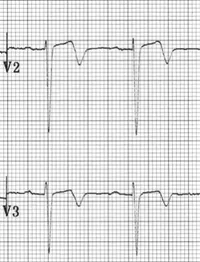
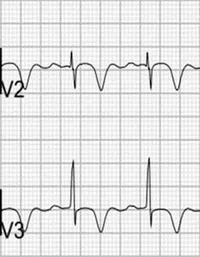
Wellens syndrome is a clinical syndrome characterised by biphasic or deeply inverted T-waves in V2-V3 (may extend from V1-V6), in the clinical context of recent chest pain that has now resolved. This is very specific for critical Left Anterior Descending artery stenosis. Wellens syndrome is a pattern seen in a pain free state and may be obscured during episodes of chest pain.
#What causes Wellens syndrome?
Wellens is a reperfusion arrhythmia, meaning that clot lysis has occurred and the deeply inverted or biphasic T-waves you see on the ECG indicate reperfusion. This is a significant example of why ECGs are important, even if the patient is pain free. Further it is a key example of why patients should have serial ECGs.
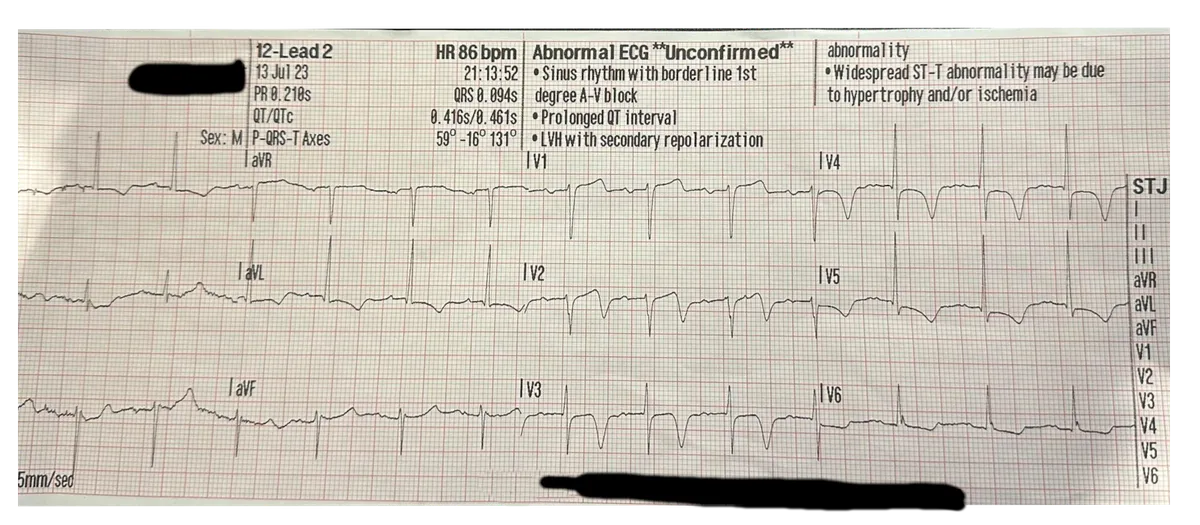
This ECG was taken on a male patient who had “epigastric” pain. The job was triaged as a 1C chest pain. The patient had taken his own GTN prior to arrival which had resolved his pain. He had a recent admission in ED for hyperkalaemia, and it was noted he was discharged with ST-elevation in V1-V3. Not so much elevation any more!
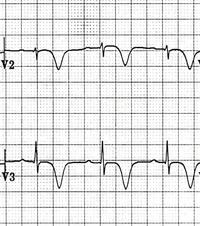
Running this ECG through an AI model trained to look for OMI, this was the result:
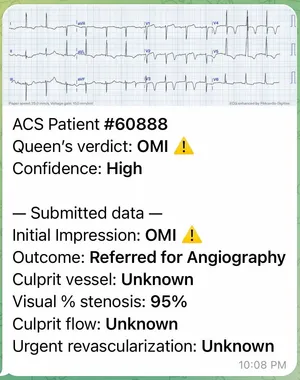
The AI model predicted a high likely hood that the patient was positive for the OMI criteria. Read more about OMI in the OMI Manifesto written by Stephen Smith, Pendell Meyers, and Scott Weingart.
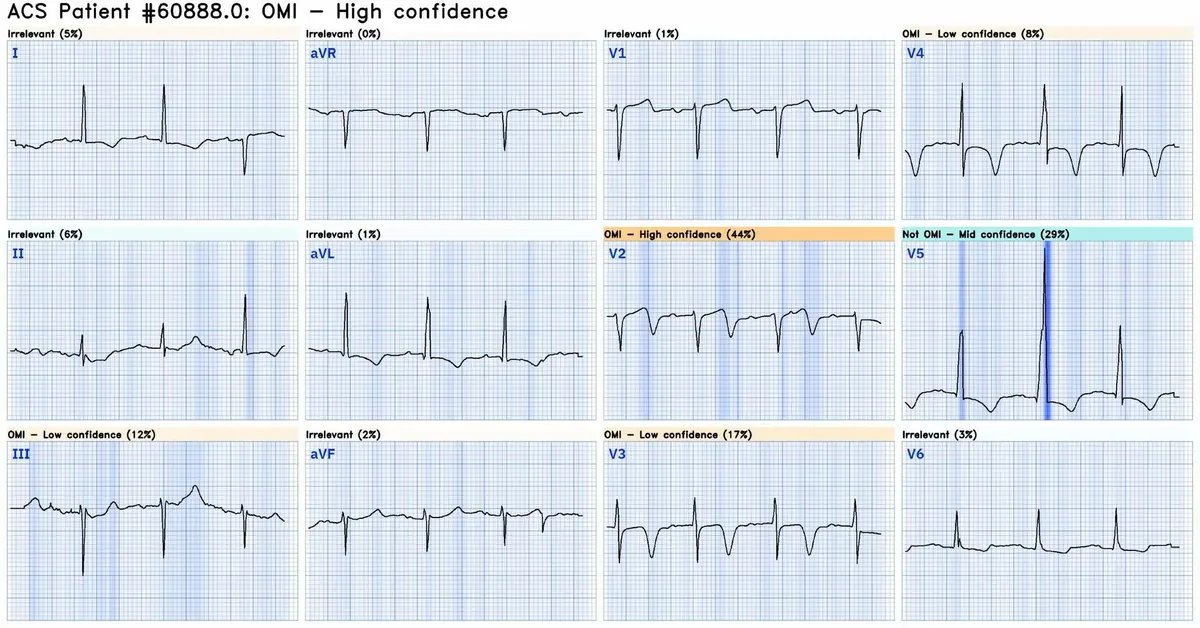
You can see a breakdown of what the algorithm is looking for in this next picture. The highlighted blue areas are what the algorithm sees, and makes it’s decision based on.
#Clinical significance of Wellens syndrome
All patients presenting with wellens syndrome are at significant risk of reoccluding. Patients with wellens syndrome require invasive therapy in the cath lab and often do poorly with medical management. This cohort of patients are at risk of further MI, or arresting.
Ask yourself, would you transmit this ECG?
Is wellens concerning considering its underlying pathology?
#Diagnostic criteria
The diagnostic criteria which is from LITFL and This paper
- Deeply inverted or biphasic T waves in V2-3 (may extend to V1-6)
- ECG pattern present in pain-free state
- Isoelectric or minimally-elevated ST segment (< 1mm)
- No precordial Q waves
- Preserved precordial R wave progression
- Recent history of angina
- Normal or slightly elevated serum cardiac markers
#Is it type A or Type B?
The type is usually time dependant. Although the T-wave morphology can be dynamic, and changes over time. Ususally they will start out as type A and progress to type B. You can read more about the T-wave progression in this LITFL article written by some much smarter people than I.
#Why is knowing about wellens important?
Wellens syndrome is important to recognise because these patients have a significantly sinister pathology underlying their presentation. Patients with wellens are at significant risk of MI and Cardiac arrest. They benefit greatly from PCI, and should be transported to a cath capable hospital.
Serial ECGs on patients are important, this is yet another example as to why.
With a little bit of knowledge, would you transmit an ECG for someone presenting with wellens syndrome?
Will you do an ECG on patients who present with ‘Epigastric’ pain or resolved chest pain?
I know I certainly would.