
#Cardiac action potential
A thorough understanding of the cardiac action potential is the key to making a link between the ECG and what is physically happening in the heart. This becomes increasingly important for those who have the ability to administer antiarrhythmic drugs.
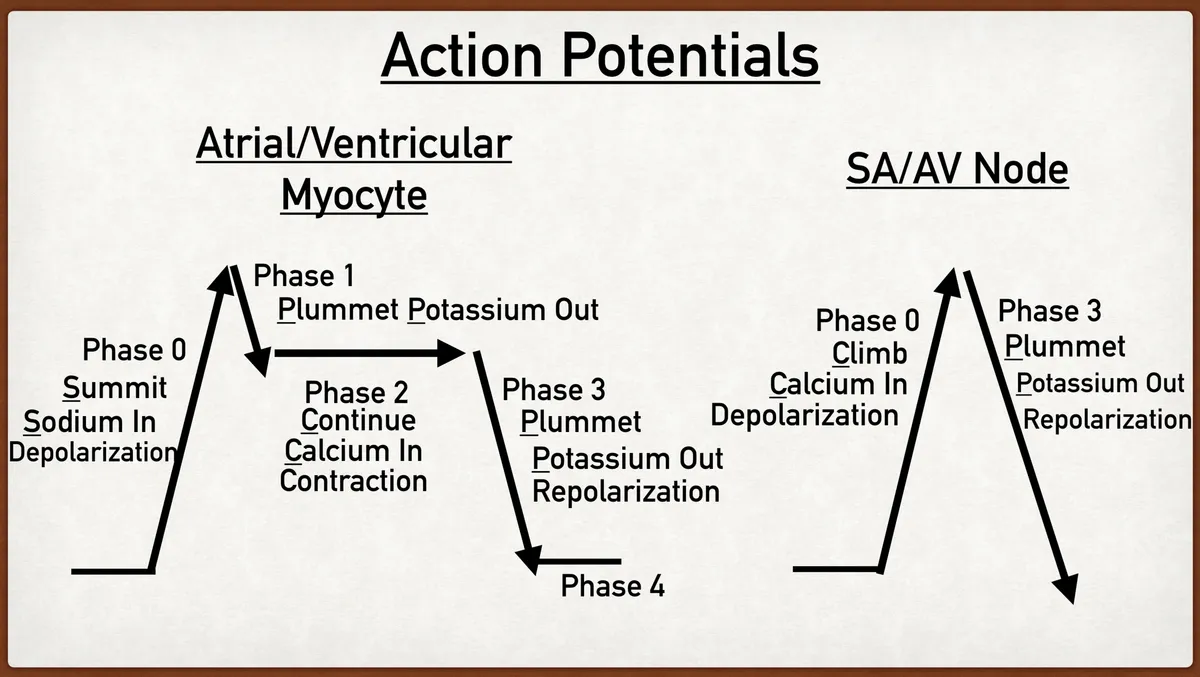
The cardiac action potential relates to the ion movements into cardiac myocytes (Atrial/Ventricular Myocytes) and cardiac pacemaker cells (SA/AV node). This is important to understand as pacemaker cells have automaticity, where as cardiac myocytes lack this ability; requiring an external stimulus.
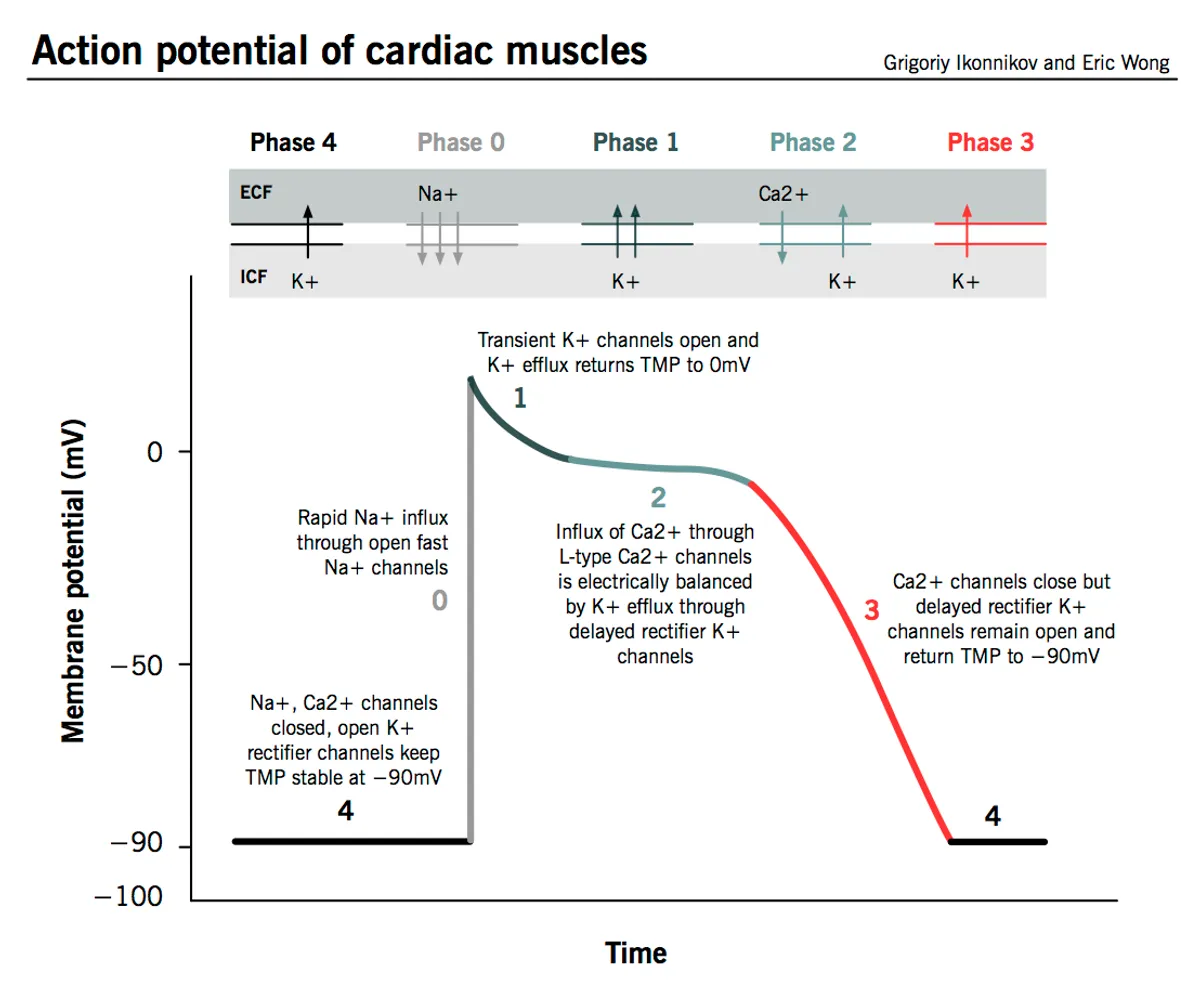
Myocyte Action potential - Source
The movement of ions across cell membranes is a complex process involving many ion channels. Sodium (Na+), Calcium (Ca2+), Potassium (K+) and Chloride (Cl-) are all involved in the depolarisation of cardiac tissue. They move across the cell membrane through selective, voltage gated, and time-dependant ion channels. This will be explained further in coverage of specific myocytes.
Resting membrane potential and threshold membrane potential are measured in mV. The rise of the transientmembrane potential from resting potential to the threshold potential is achieved through the movement of ions across the cell membrane. This is important to understand, especially in the presence of electrolyte disturbance. This is the process of depolarisation of cardiac myocytes.
#Cardiac pacemaker cells
As mentioned previously, pacemaker cells have automaticity. This means they do not require external stimulation to initiate their action potential. They are capable of self initialisation of depolarisation in a rhythmic fashion.
Depolarisation of pacemaker cells is unique. The sequence for depolarisation of pacemaker cells:
- Slow Na+ channels slowly raise the transientmembrane potential above -60 mV (Called the funny current).
- At -55 mV, Low-voltage Ca2+ channels open, continuing to slowly increase the transient membrane potential.
- At -40 mV, the threshold potential, High voltage Ca2+ channels open, depolarising the pacemaker cell, overshooting to +40 mV.
- K+ rectifier channels open, returning the membrane potential back to -60 mV, the resting potential.
Pacemaker cells have dominance over cardiac myocytes. Meaning they initiate stimulus in the heart, passing this stimulus to other myocytes through gap junctions.

#Cardiac Myocytes
Cardiac myocytes unlike pacemaker cells, require external stimulus to begin depolarisation. The action potential in typical cardiac myocytes is composed of 5 phases. Starting and finishing with phase 4.
The ion influx and efflux is much more complex in cardiac myocytes compared to pacemaker cells. The resting membrane potential of cardiac myocytes is around -90 mV. Much lower than the pacemaker cells -60 mV.
To enhance your ability to remembering the process of ions in the cardiac action potential, I have stolen a little catchphrase from EZmed Summit, Plummet, Continue, Plummet - Sodium, Potassium, Calcium, Potassium. This will become clearer below.
#Phase 4 - Resting phase
- Membrane potential of -90 mV
- Slow influx of Ca2+ through gap junctions increase membrane potential to the threshold potential -70 mV
#Phase 0 - Sodium in - Summit
- Threshold potential is met at -70 mV
- Rapid influx of
Sodiumthrough Voltage-gate and fast Na+ channels - Long opening Ca2+ channels open around -40 mV
- Rapid rise of membrane potential to a
Summitof a +20 mV - K+ channels open, allowing outwards flow of potassium
- Voltage gated Na+ channels close
#Phase 1 - Potassium out - Plummet
- Voltage gated Ca2+ channels open
- Inwards movement of Ca2+ is important for myocyte contractility
- K+ channels continue with outwards flow of
Potassium
#Phase 2 - Calcium in - Continue
- Ca2+ and K+ act to balance the membrane potential
- Ca2+ influx is responsible for myocardial contraction - which happens during this phase
- Cl- channels are activated and Cl- is moved into the cell
- The
continuationof this process creates the plateau phase
#Phase 3 - Potassium out - Plummet
- Relaxation phase
- Ca2+ channels close
- K+ channels remain open - Outwards movement of
Potassiumcontinues - Ion pumps move Ca2+ out of the cell
- Outwards movement of positive ions such as K+ and Ca2+ slowly returns the membrane potential to the resting potential of -90mv.
- Repolarisation has occurred and the cell is ready for another stimulus.
#Why is this important?
A fundamental knowledge of the cardiac action potential is important to strengthen your understanding of ECG basics. Many drugs act on the the ion channels found in the heart, particularly antiarrhythmics. Pharmacological toxicity can have profound effects on the cardiac action potential for example Calcium channel blockers, Beta Blockers, or other drugs which cause Na+ or K+ blockade.
Electrolyte disorders effect the function of the heart and can often be seen on ECGs. This is most often seen in conditions such as Hyper/hypokalaemia.
Some disorders of ion channels can lead to long QT syndrome and Brugada syndrome.
Overall, having a solid understanding of the cardiac action potential will enhance your ability to diagnose and understand ECG changes, and how certain conditions effect the heart.
#References
- http://www.pathophys.org/physiology-of-cardiac-conduction-and-contractility/
- https://www.ezmedlearning.com/blog/actionpotential
- https://www.osmosis.org/learn/Action_potentials_in_myocytes
- https://derangedphysiology.com/main/cicm-primary-exam/required-reading/cardiovascular-system/Chapter%20011/fast-voltage-gated-sodium-channels-cardiac-muscle
- https://www.frontiersin.org/journals/cardiovascular-medicine/articles/10.3389/fcvm.2019.00054/full