Calcium channel blockers

Joshua Foster @facebook
#Calcium channel blockers (CCB)
#Preface
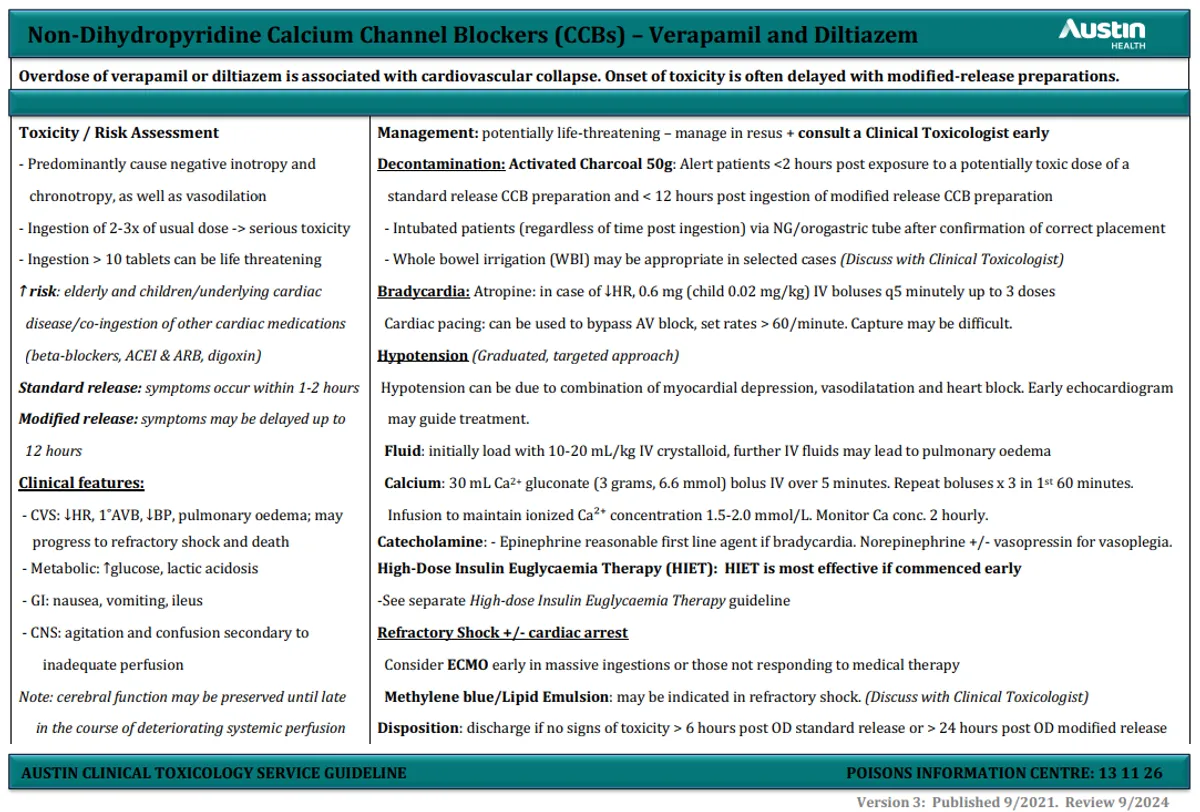
CCBs are widely used in anti-hypertensive therapies. In overdose, CCB’s exhibit a profoundly toxic effect. Acting to block calcium uptake in the myocardium and vascular smooth muscle, toxicity can quickly lead to cardiovascular collapse and death.
#Mechanism of action
CCBs are classed as dihydropyridine and non-dihydropyridine types. All CCBs inhibit voltage-gated L-type calcium channels in the myocardium and vascular smooth muscle. Voltage-gated calcium channels are responsible for for excitation-contraction coupling of skeletal, smooth, and cardiac muscles. Blockade of calcium influx therefore directly decreases vascular smooth muscle and cardiac muscle contraction. They also play a large role in the conduction of cardiac pacemaker signals. At therapeutic doses, dihydropyridine’s are selective for blood vessels, where as non-dihydropyridine’s act both on reducing vascular contraction (peripheral resistance) and have specific effect on cardiac tissue. Non-dihydropyridine’s further depress myocardial contractility, reduce sinus node firing rate and AV-node conduction.
Dihydropyridines
- nifedipine
- felodipine
- Amlodipine
Non-Dihydropyridines
- diltiazem
- verapamil
Non-Dihydropyridines are the most lethal CCBs due to their non-selective nature, although dihydropyridines loose receptor selectivity in large overdose. The coformulation trandolapril (ACE inhibitor) + verapamil will have profound effects as congestion will potentiate the effects of overdose.
#Clinical presentation
Cardiovascular
- Sinus bradycardia, conduction delays (First-degree heart block, junctional and idioventricular rhythms)
- Hypotension due to bradycardia, myocardial depression and vasoplegia
- Cardiogenic shock
- Pulmonary oedema
CNS
- Drowsiness
- Confusion
- Agitation
- Seizure
Metabolic
- Hyperglycaemia
- Acidosis
Onset of symptoms
- Immediate-release formulations: Symptoms typically occur within 1-2 hours of ingestion
- Extended-release formulations: Symptoms may be delayed, occurring up to 12-24 hours after ingestion
#Prehospital Management
Symptomatic management of CCB overdose is the forefront of pre-hospital care. Rapid transport to a tertiary hospital is necessary.
Bradycardia
- Atropine - 600mcg undiluted bolus, RPT: 1min, Max Dose: 3mg
- Adrenaline - 50mcg bolus 1:1000, RPT: 1min, NO MAX
- Adrenaline infusion
- Calcium Gluconate 10%
- Trans cutaneous pacing - May be difficult to obtain capture
Hypotension
- 20ml/kg Bolus, whilst indicated, NO MAX
- Calcium Gluconate 10%
Calcium gluconate
Calcium gluconate can have useful temporising effects on HR and BP. Calcium gluconate is only indicated for hyperkalemia in NSWA.
A VCP will need to be completed if calcium gluconate is used in the setting of CCB overdose.
Read more Here
Early activation of ICP resources would be of great benefit. Although not always available, it is always advised to ask!
#References
- CCBs - Australia Prescriber
- CCB poisoning - Therapeutic guidelines
- Calcium Channel Blocker Toxicity - LITFl
- Austin Clinical toxicology guidelines
- EMcrit - CCBs